


The Perplexing Question of Birth Control When You Have PMDD
A conversation with Dr. Andrea Rapkin, director of the UCLA Pelvic Pain Clinic

Good afternoon everyone! This issue is a little late, but cycles vary and so does…The Monthlies? My friends and family have told me I’ve vastly exceeded my quota of period jokes, but I maintain if you have PMDD you have to find your kicks and giggles somewhere.
For this month, I chatted with Dr. Andrea Rapkin about her 2019 review of the academic literature on birth control options for people with PMDD. Going on birth control can be a tricky proposition for anyone with a hormone sensitivity.
Dr. Rapkin is the director of the UCLA Pelvic Pain Center and author of two books on PMDD. In her review, Dr. Rapkin sums up what we currently understand about how different types of birth control impact PMDD’ers.
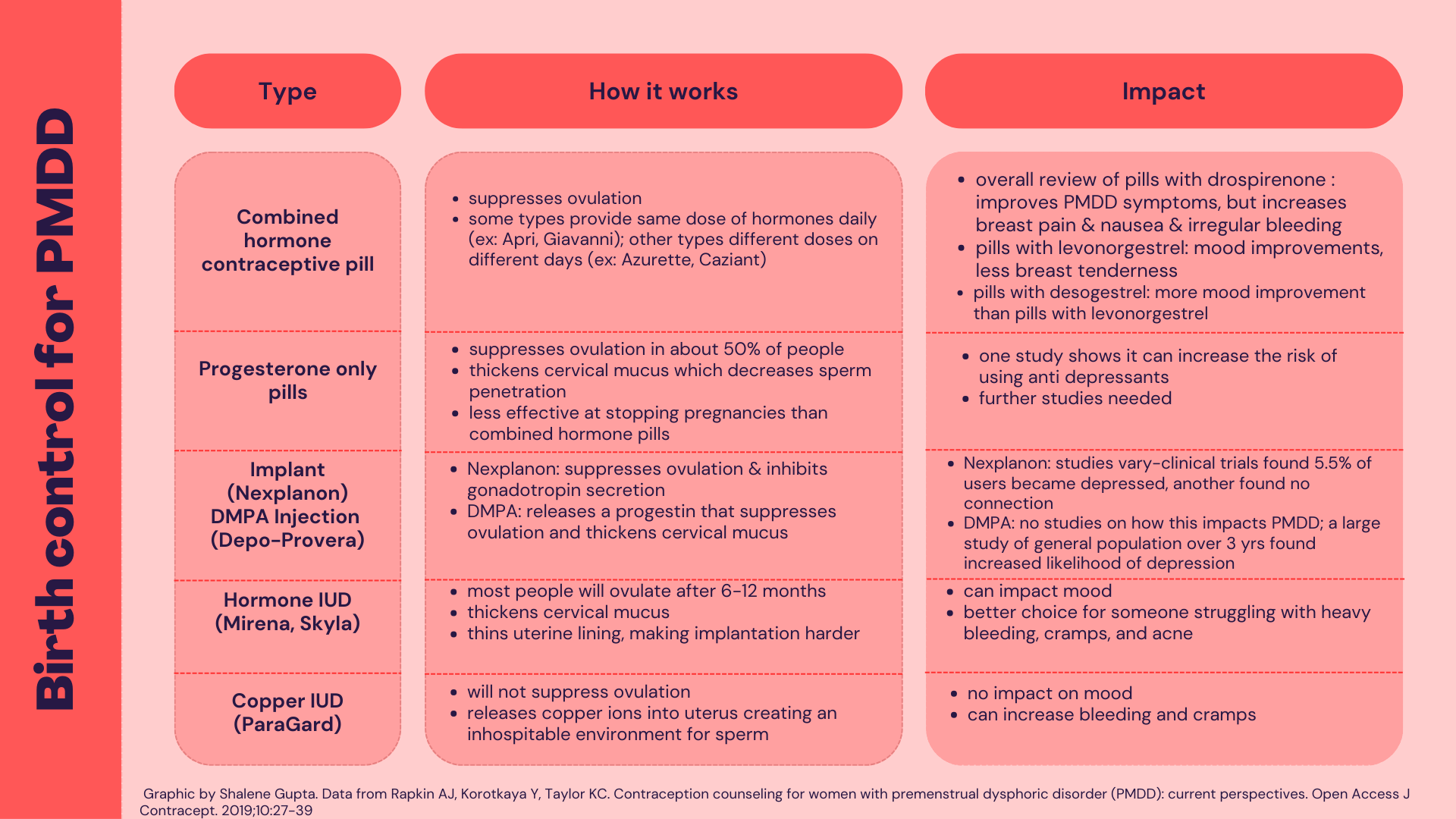
At the highest level, combined hormonal contraceptives are the best option for people with PMDD. Combined hormonal contraceptives are pills that contain estrogen and a progestin—a synthetic form of progesterone. Dr. Rapkin’s review covers studies on pills that use three different types of progestins: drospirenone, levonorgestrel, and desogestrel. Studies show all three improve PMDD symptoms but to different extents and come with side effects.
I’ve summarized the review in the graphic below, and Dr. Rapkin provides an overview in our conversation. The paper is available for free and it’s well worth combing through if there’s a specific birth control you have questions about. Note: you will have to look up the formulation of the birth control, since the paper does not use brand names. I have attempted to provide common brand names, but there are too many to capture.
Yaz, which has 3 mg drospirenone/20 mcg ethinyl estradiol, is the only FDA approved birth control for PMDD. It the most evidence for helping PMDD’ers with their symptoms. As a side note, Yaz was terrible for me, but I’ve spoken to many people it helped. My symptoms were wiped away with a levonorgestrel pill (Seasonique)—but so was my libido. I’m currently trying Apri, which has desogestrel. So far it hasn’t been as magical as Seasonique, but much better than Yaz. Keep in mind: what works for one person may not work for you. Track your symptoms across one or two cycles carefully and consult your doctor if you have any concerns.
SG: Why did you write this review?
AR: Aside from pregnancy risks, hormonal contraceptives can help with cramps, heavy bleeding, and endometriosis. They can also help with acne. The review is important because many women who have PMDD don't tolerate hormonal contraceptives. I wanted to see what the literature showed in terms of actual studies and cover what might be useful contraception information for women with PMDD.
SG: In general, if you have PMDD, what’s your best option for birth control?
AR: Theoretically if you block ovulation, you should prevent PMDD. But practically speaking it doesn't always work that way. The progestin in the birth control pill may not be tolerated and may create some of the same changes in the brain that progesterone does with ovulation.
If someone hasn’t tried an oral contraceptive for PMDD, there’s one that’s been approved through the FDA: it’s 20 micrograms of ethinyl estradiol and 3 milligrams drospirenone that comes in a 24 day active pill and 4 days off. You can also skip the four days off. (Editor’s note: Yaz).
If someone has tried Yaz and another combined oral contraceptive option and neither have worked, we are probably looking at a copper intrauterine device (IUD). With the copper IUD, you're going to have potentially heavier and more painful menstrual periods.
It is possible for someone who has menstrual pain or heavy menstrual bleeding to try the levonorgestrel IUD (hormonal IUD). Some women with PMDD will still be sensitive to the low level of levonorgestrel in the IUD. This would be a trial with the idea that for up to six months there is more hormone in the bloodstream.
Still, the hormonal IUD might be worth a try because with the copper IUD you're going to have potentially heavier and more painful menstrual periods. The hormone IUDs are very good for menstrual pain and for heavy menstrual bleeding.
SG: How long should you give a birth control before you stop it because it’s not working for you?
AR: In the studies, the improvement was fairly immediate. If you started the birth control on first day of menstrual cycle, give it between one to two cycles. Keep in mind, there’s some irregular bleeding that can occur within two to three months. With mood symptoms it’s hard to say—if after two months the symptoms haven’t improved, they probably aren’t going to get better. However, the hormonal IUD is worth trying for up to six months as long as you can tolerate the symptoms.
SG: What about the morning after pill? How does something like Plan B impact PMDD—what should you expect from your cycle if you take Plan B?
AR: If you’ve had sex and think you’re near ovulation, I certainly would encourage using Plan B, rather than going with nothing. Plan B works to interfere with ovulation, not implantation of a fertilized egg into the uterine lining.
However, it is a significant dose of a progestin. There maybe PMDD symptoms and they might get worse, but not invariably. I wouldn’t withhold Plan B from people with PMDD.
The other option, if you are around time of ovulation, is to go to a healthcare provider and get a copper IUD that acts a morning after. The copper IUD combined with ibuprofen can bring cramping back down to a normal range.
SG: How do birth controls react with SSRIs?
AR: There’s no impact. The only major interaction with hormonal birth control are some of the anticonvulsants which are sometimes used as mood-stabilizers in women with bipolar disorder.
SG: Many of us have doctors who aren’t well versed in PMDD. What tips do you have for us when we’re trying new birth controls?
AR: After you take hormonal birth control do DRSP (Daily Record of Severity of Problems) rating. Print them out and bring them to your doctor so you can back yourself up with data. A lot of times patients hand me their phones and it’s hard to scroll through, plus I feel like I’m handling something private.
I don't know why some doctors don’t know what PMDD is. It’s in our residents’ curriculum. It's in our medical students’ curriculum, but it's not something that they absorb. It’s really unfortunate.
That’s all, folks!
If you have a suggestion for future editions, questions, or comments feedback you can leave a comment or messages me.
If you found this helpful, please share it with a friend!
I noticed you advised not to use progesterone for PMDD and many folks have tried a cream and say they’ve had some success. Does progesterone present complications in all forms (creams, bio-identical etc)?